There is lots of evidence that the premature brain is particularly susceptible to injury that can result in long term problems including learning, behavioural and motor disabilities, and that it develops differently in the ex utero environment than it does in the womb. I'm looking at magnetic resonance brain images of preterm (i.e. premature) babies who were scanned at term equivalent age and comparing these to images from term born babies. I'm not using conventional MRI to compare them though, but with a technique called diffusion tensor imaging (DTI), where the image intensity is dependent on the diffusion properties of water within the tissue. Water molecules are restricted by microstructural boundaries including cell membranes and axonal tracts, which become more numerous as the brain develops with age. DTI therefore allows you to assess brain microstructure, and so may allow the visualisation of brain lesions in preterm infants before they are seen with conventional MRI. However, due to the way DTI data is acquired, it's susceptible to severe image distortion in a particular direction. I'm working on ways of computationally correcting this post-scan, so that the data is good enough to allow comparisons. I'm also trying to put all of the images into a common reference frame, so that the comparisons can be objective, unlike region of interest analyses.
It's probably easier to explain this last part if I show you a couple of pictures. In both images, which are taken from the same infant, a T2 MRI slice is on the left of the dotted line, and a corresponding B0 slice is on the right. I am trying to put them into the same reference frame. 'Before' shows alignment before I applied the registration, and 'After' shows alignment after registration. The yellow arrows reflect the tissue displacement that has taken place. It doesn't yet work as well all the time, but I'm hoping to improve that! Once I’ve got all the brains into a common reference frame I can begin comparing groups of preterm and term infants.
Anyway, I'd better hear off - it's our Christmas party. Should be fun!
All the best,
Moc
Before (structures misaligned)

After
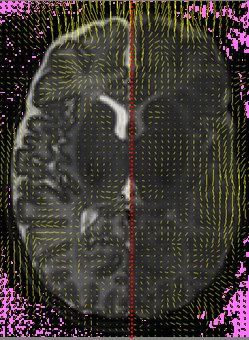
P.S. Please ignore all that pink noise - it just appeared when I tried to upload the images to blogger.
